
1Dipartimento di Elettronica, Informazione e Bioingegneria, Politecnico di Milano, 2Fondazione Istituto Farmacologico Filippo Serpero, Milano, 3IRCCS San Raffaele Pisana, Tosinvest Sanità, Roma, and 4Department of Mechanical, Chemical and Materials Engineering, Università di Cagliari, Cagliari, Italy
Objective: Sex-specific medicine requires understanding of the specific therapeutic needs and patho-physiology of men and women. In these terms, we investigated sex-related differences in the gait kinematics of patients with Down syndrome.
Design: Retrospective observational cohort study.
Subjects: A sample of 230 patients (103 females) aged 7–50 years underwent a standard gait-analysis test from 2000 to 2015.
Methods: Spatiotemporal gait parameters and synthetic indexes were computed as Gait Profile Score (GPS) and pelvis/lower limbs as Gait Variable Scores.
Results: Although speed, normalized step width, %stance and %swing were similar, in female patients step length was shorter and GPS was higher than in male patients, with no significant effect of age, speed and body mass index. Sex-specific features were found at the pelvis, hip and knee level (sagittal plane), and at the ankle level (transverse plane).
Conclusion: Overall, in people with Down syndrome, the gait function of females tends to be more impaired than in males, with the exception of foot progression. Therapists should consider these differences when evaluating the severity of gait impairment and designing rehabilitation strategies.
Key words: Down syndrome; sex; gait analysis; kinematics.
Accepted Oct 23, 2018; Epub ahead of print Dec 19, 2018
J Rehabil Med 2019: 51: 00–00
Correspondence address: Matteo Zago, Dipartimento di Elettronica, Informazione e Bioingegneria, Politecnico di Milano, Piazza Leonardo da Vinci 32, IT-20133 Milano, Italy. E-mail: matteo2.zago@polimi.it
In Down syndrome, gait function tends to be more impaired in females than in males, even when taking into account the confounding effects of age, gait speed and anthropometrics. Therapists should be aware of these differences when evaluating the severity of gait impairment and in designing rehabilitation strategies.
Sex-specific medicine, a global trend in modern healthcare, requires detailed understanding of the different signs, pathophysiology and therapeutic needs of males and females (1). Little is known about sex differences in the gait function of patients with Down syndrome (DS). DS is a chromosomal aneuploidy that produces disruptions in various body systems, including musculoskeletal function, and delayed neuropsychomotor development (2). In particular, ligament laxity, osteoporosis, and muscle hypotonia in the lower limbs critically affect postural control and mobility (3–5): gait function is characterized by reduced speed, reduced step length and increased step width, balance deficit, joint instability (increased mediolateral centre of mass displacement) and energetic inefficiency (6–8). Alterations in joints kinematics include excessive pelvic tilt, external hip and tibial rotation, increased hip flexion and knee flexion during the stance phase, with associated limited range of motion, abnormal foot rotation and reduced propulsive action of the ankle plantarflexors (4, 9, 10).
With respect to healthy women, age-matched healthy men generally walk at higher speed, take longer steps with consequent reduced cadence (11), and show joint kinematics peculiarities, driven by both morphological and social factors (12).
In the event of musculoskeletal (13) or neurological diseases (14, 15), sex-specific gait patterns may be enhanced or modified. We hypothesize that sex-related differences could also be present in people with DS. This paper characterized the gait kinematic phenotype of males and females with DS. As the gait function is, to some extent, trainable in people with intellectual disabilities (5), distinct features may suggest redesigning or customizing rehabilitation and physical treatment procedures.
A sample of 230 patients diagnosed with DS (103 females, 127 males) were recruited for this retrospective cohort study from 2000 to 2015. A total of 44 patients (22 females, 22 males) aged 6–12 years, 39 (16 females, 23 males) aged 13–18 years, 134 (60 females, 74 males) aged 19–40 years and 13 (5 females, 8 males) aged > 40 years were analysed. Inclusion criteria were: diagnosed pure trisomy 21 chromosome abnormality, no clinical sign of dementia, and no previous surgery. All individuals could understand and complete the gait test and walk independently. Patients or legal guardians signed a written informed consent prior to participation. This study was approved by the ethics committee of the IRCCS San Raffaele hospital (protocol #17/17) and conducted according to the Declaration of Helsinki.
Gait tests were performed within the gait analysis laboratory of the IRCCS San Raffaele Hospital (Rome, Italy), equipped with a 12-camera motion capture system (Elite 2002, BTS, Milan, Italy); 22 spherical reflective markers were placed on patients’ body according to the Davis protocol. Participants were requested to walk at comfortable speed 6 times on a 10-m lane. Anthropometrics and intellectual quotient (IQ) were obtained through the Wechsler’s Intelligence Scale for Children (WISC-III) and Adult Intelligence Scale (WAIS-R), according to participant’s age (16).
The following spatiotemporal gait parameters were obtained: speed, cadence, step length and step width (normalized by body stature), %stance, %swing. Gait Profile Score (GPS) and Gait Variable Scores (GVSs) relative to pelvis and lower limbs were computed to account for the distance of angular kinematic from a healthy reference population (17), on a global and joint-level perspective. A GPS ≤ 7° is considered normative for healthy people (18). Variables were submitted to multivariate analyses of covariance (MANCOVA) to test sex-related differences, taking age, speed and BMI as covariates. A significance level of 0.05 was implemented throughout.
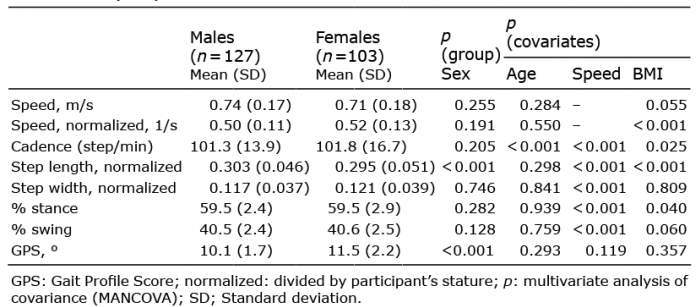
IQ ranged from 33 to 91 (first quartile 60, third quartile 73), with no sex differences (p = 0.616) nor age/speed effect (p = 0.059 and p = 0.360, respectively). In both males and females BMI increased, and cadence decreased with age (sex factor, p > 0.05, age factor: p < 0.001). Speed, normalized speed, step width, % stance and % swing were similar in male and female patients (p > 0.05, Table I), while step length was slightly shorter in females (p < 0.001). In female patients, GPS was, on average, 12% higher (p < 0.001) with no significant effect of age, speed and BMI; the GVS of pelvic tilt (p < 0.001), pelvic rotation (p = 0.021), hip flexion (p < 0.001), and knee flexion (p = 0.033) were higher than in males (Fig. 1). The GVS of foot rotation was higher in males (p = 0.046).
Table I. Sex-related differences (mean and standard deviation on the whole sample) in gait parameters, corrected for the effects of age, gait speed and body mass index (BMI)
Fig. 1. Sex differences in joints Gait Variable Score (GVS). A/P, Rot and U/D: pelvic tilt, rotation and obliquity, respectively; F/E: flexion/extension. Significant differences between male and female patients with Down Syndrome: *p < 0.05 and **p < 0.01, corrected for the effects of age, speed and body mass index (BMI).
This study suggests that, in people with DS, global gait function tends to be more impaired in females than in males. Sex-specific features were found in the sagittal plane at the pelvis, hip and knee level, and in the transverse plane at the pelvis, hip and foot level.
Overall, patients’ GPS was > 10°, denoting a general picture of impaired gait (18). The largest GVSs (hip and knee flexion, hip and foot rotation) matched the common gait phenotype of patients with DS (4, 9, 10).
Male and female patients with DS showed similar cadence and normalized step width, as in (19), but shorter step length. This agrees with previous observations showing that healthy females walk with a shorter step length (12, 20), also when taking dimensionless (normalized) measures (21). Gait speed was comparable in males and females, together with BMI and IQ. As speed has a substantial effect on gait kinematics (11), the observed differences in the motion of the joints cannot be ascribed merely to speed-size mismatches, nor to cognitive function. Rather, a sex-specific movement pattern emerged from multi-plane joints motion: in females, sagittal-plane joint kinematics was more altered at the pelvis, hip and knee level; pelvis and hip rotation and pelvis tilt were also impaired; an opposite trend was found on foot progression, as the corresponding GVSs was higher in men.
These results further confirm recent observations showing that women with DS tend to have larger hip flexion at late stance and reduced knee flexion at early swing, while men showed larger foot extra rotation at late swing (15). Hip and knee flexion deficits are probably associated, as in healthy women, with weaker abdominal (20) and hip flexor (22) muscles. Altered foot progression is common in DS due to flatfoot (4), and its prevalence is higher in male patients (23): this may explain the higher foot progression GVS observed in males, and it is reinforced by previously observed sex-related differences in plantar pressure distribution among children and adolescents with DS due to a different distribution of fat mass (24).
Synthetic indexes (such as GPS and GVSs) inherently lack focus on the angular kinematics of joints throughout the step cycle (25), as high GVS values are uninformative about the signs of deviation (increased or diminished joint angle). However, they allowed the gross kinematic differences between males and females with DS to be examined. Future longitudinal analyses would allow specific trends in the gait function over the entire lifespan to be determined, potentially due to sex- and age-related comorbidities, such as osteoporosis, early menopause and muscle hypotonia and, most importantly, the relationship between sex-specific gait impairments and fall rate.
In summary, spatiotemporal parameters and synthetic gait indexes showed that males and females with DS exhibit different joint patterns during gait, as observed previously in healthy individuals due to a combination of intrinsic morphological and musculoskeletal factors (12, 21): pelvic tilt, hip and knee flexion, and hip rotation were more altered in females; however, foot progression, which constitutes a specific trait of this pathology, was more impaired in men.
This study impacts on both diagnostics and rehabilitation: in instrumented gait analysis and functional evaluations, female and male patients with DS are often pooled. There is evidence that therapists and clinicians should be aware of specific features when evaluating the severity of gait impairment and designing customized rehabilitation strategies.
This project was partially supported by an unconditioned Research Grant supplied from the “Filippo Serpero Foundation”, Milan, Italy.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize